Sweden is a country located in Northern Europe. It has an area of 450,295 square kilometers and a population of approximately 10 million people. The ethnic composition of Sweden is largely homogeneous, with the largest group being Swedish (86%), followed by Finnish (5%), and other European (3%). The majority of the population are adherents to Christianity, with around 70% following the religion and the rest being either Muslim or non-religious. Education is compulsory for children up to the age of 16 and the literacy rate is estimated to be around 99%. The official language is Swedish but there are also many other languages spoken throughout the country such as Finnish, Sami and Meänkieli. The capital city Stockholm has an estimated population of over 1 million people making it one of the largest cities in Sweden. Check hyperrestaurant to learn more about Sweden in 2009.
Social conditions
Sweden – like Norway and Finland – has not had a period of feudalism. A majority of the population have been free farmers with families. The need for social intervention was met during the Middle Ages by the Catholic Church. The Reformation diminished the Church’s opportunities for relief activities. At Västerås Parliament in 1527, the king (the state) undertook to provide for the care that the church could no longer afford; but for a long time it was not much. It was not until the 17th century that the state began to establish hospitals for mental and venereal diseases, which eventually developed into county court and in 1862 were placed under the then county councils. Public health care was also started by provincial doctors.
During the 19th century, the population increased rapidly. Despite increased supply opportunities, the need for help became greater as more and more people became dependent on cash income. The relief activities which the parishes had carried out even after the Reformation were now regulated by the 1847 Poverty Regulation (see Poor Care). From 1884 onwards came proposals for social insurance, which, however, were not implemented until during the 1910s. At that time, the National Pension was decided in 1913 and occupational injury insurance in 1916, but also social welfare laws: Alcoholics Act 1913 and the new Poverty Law 1918, 1924 supplemented with a child welfare law. Regulation and state subsidies for voluntary health insurance were introduced in 1931 and for unemployment insurance funds in 1934. Check to see Sweden population.
During the 1930s, the social policy discussion was first dominated by the unemployment policy and later by the family policy. The reform work was interrupted by the World War 1939, but it was free maternity care, free health control at maternity and child care centers and a small maternity allowance. It was also built “children’s home” for low-income families. After the war came new major reforms, mainly the substantially improved national pensions and the general child allowances, both from 1948. However, general health insurance was not introduced until 1955. An important change was that the elderly care was released from the poor care from 1947. During the 1950s, the alcohol rationing was abolished (Br.) introduced in the 1910s, while the state monopoly on sales (Systembolaget) was maintained. Municipal leisure activities for youth and state grants to youth organizations were also introduced.
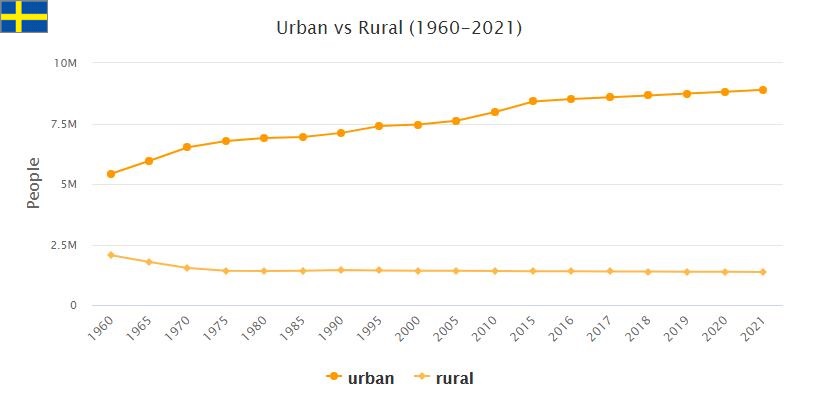
The big issue in the 1950s was otherwise the supplementary pension. ATP (from 1963) has resulted in a significant leveling of pensions. In the 1950s and 1960s, immigration to the urban areas increased sharply, which was accelerated by a conscious labor market policy. The development meant that married women were increasingly working outside the home. This increased the need for municipal childcare, which in turn required more labor, which was often made up of women. The same was true of the concurrent development of home care services for the elderly.
Overall, the economic and social development meant that Sweden was probably around the world around 1970 in terms of a high and evenly distributed standard of living, including security to maintain it in the event of illness, unemployment and old age. Social care was modernized through a law on social services, which from 1982 replaced the previous care laws. Compensation levels of social benefits were greatly increased.
Welfare and poverty
Welfare in Sweden is more evenly distributed than in most other countries. But even though there is a relatively even distribution of income both before and after tax, there are significant differences, which have increased in recent decades after the equalization that took place during much of the 20th century.
There are major differences between those who have different education and professions and between those who have work and those who do not have it. People who have come to Sweden as refugees in recent years generally initially have low incomes, which can partly be explained by the fact that it takes a long time to establish themselves in the Swedish labor market with its demands for knowledge of Swedish and education. Estimates of the welfare index (HDI) for 2014 show that Sweden was in 14th place out of a total of 188 countries and territories in the world.
Insurance
For a long time, Sweden has well-developed social insurance that provides compensation for illness, work injuries, disabilities, childcare and old-age pension. The first two were introduced more than 100 years ago; the riksdag decided on a general old-age pension in 1913 and an occupational injury insurance in 1916. These and other social insurance policies have changed on several occasions. The basic principle is that the state compensates for the loss of income from work. There is also a compensation for one who has had low or no income from work. An income ceiling regulates that income above a certain level is not compensated.
In addition to social insurance, there are supplementary benefits determined by agreements between the social partners; insurance agreement. They increase the compensation for income under the ceiling and also provide compensation for income portions above the ceiling in social insurance. The vast majority in the Swedish labor market are covered by the contract insurance. Exceptions comprise a significant portion of those who are self-employed persons who have not taken out insurance and some employees whose employers have not signed collective agreements or equivalent insurance for their employees.
There are supplementary private insurances, e.g. private pension insurance. However, they play a lesser role in Sweden than in many other countries, such as the USA.
Labor market, trade unions and pensions
Labor force participation is high in Sweden. Compared to most other highly developed countries, the proportion of employed persons is particularly high among the elderly. Characteristic for Sweden is also that the difference between men’s and women’s labor force participation is relatively small. However, there are differences in working hours – women work more part time. This contributes to women receiving, on average, significantly lower pensions than men.
Unemployment was very low in Sweden for several decades, but increased dramatically during the economic crisis in the early 1990s. It dropped during the late 1990s but still remains at a significantly higher level than before the 1990s. Part of the explanation is a rapid restructuring of the Swedish business community, which has meant increased demands on those who are employed.
The proportion of employees who are members of a trade union organization is high in Sweden, although it has declined somewhat over the past decade. Most unions are members of one of three top organizations: LO for workers, TCO for officials and Saco for academically educated. There are also some trade unions that do not belong to any top organization. Employers are organized by sector (private, municipal, state). Wages are determined in collective agreements. In Sweden, there are no minimum wages set by the state as in, for example, the US and Germany. Unemployment insurance is closely linked to the trade unions through unemployment funds. In addition, there are various supplementary reimbursements through contracts or supplementary insurance.
There is currently no statutory retirement age in Sweden. The pension from the general pension system can be deducted at the earliest from the age of 61, but there is no upper limit on when it must last start to be taken out. The annual pension becomes higher the later it starts to be taken out. The Employment Protection Act (LAS) provides protection up to the age of 67. However, many begin to withdraw their pension at the age of 65, which was the previous retirement age. For some years now, there has been a political debate about raising the various age limits and thus trying to raise the actual retirement age.
Child allowance and childcare
A general tax-free child allowance was introduced in 1948. It is not income tested and is the same for all children, but with a multi-child allowance (higher allowance per child if more than one child). Unless otherwise decided, the child allowance is shared equally between the parents.
For parents, there is the right to leave with compensation for the care of children, so-called VAB. Relatives such as grandparents can grieve. The scope of the leave that is compensated has been expanded in various stages. There is also a right to compensation in the absence of work for the care of sick children. Women’s withdrawal from parenting days is high, about three-quarters. Men are taking more and more parenting days off, but the change is slow.
Preschool activities expanded rapidly from the late 1960s onwards. There is a right to a place at preschool from the age of one child. From the age of six there is a preparatory school year. The expansion can be seen as part of a policy to enable both women and men to work. Another part of this policy was the introduction of special taxation on spouses.
Health insurance and health care
The average life expectancy in Sweden is 84.0 years for women and 80.3 years for men (2015), which is among the highest in the world. Infant mortality is low. Healthcare in Sweden is a regional municipality and mainly financed through an income tax to the region. There are fees for those seeking care, but they are low and there is a high cost protection for those who have multiple care cases during one year. In the same way, there is a high cost protection in the case of medicines prescribed by doctors.
Equality
Women and men have the same statutory rights, but there are significant remaining differences in some areas. In political bodies and parishes such as the government, parliament and the municipal council, there is now about the same proportion of women and men. In the Riksdag, the goal of an even gender distribution was reached in 1994, when the proportion of female members was 40 percent. After the 2006 election, the distribution was almost even, and then reversed slightly to 45 percent after the last election.
In the case of top positions in business (managers and board members), the proportion of men is significantly higher than the proportion of women, although there is a slow leveling. In Norway, there is a law that the proportion of women (and the proportion of men) should constitute a certain minimum proportion on the boards of larger companies and discussion is ongoing about the introduction of such a law also in Sweden.
Women and men are to a large extent employed in various parts of the labor market. Wages are higher in the professions where the proportion of men is high. Even a comparison of women and men in the same profession shows that men have higher wages – the differences are smaller, however.
Crime and punishment
The penalties are relatively low in Sweden, but not for drug-related crimes. Overall, the number of people taken into custody after being sentenced to prison has decreased over the past decade, while the number admitted to drug-related crimes has increased. The great majority sentenced to prison are men. In 2016, the legislation on terror-related crimes was tightened.